Function of the Pons and Pons Anatomy
Children who are diagnosed with DIPG often experience varying clinical symptoms. Families are sometimes left wondering why their child exhibits a particular symptom, while another child may not. Additionally, families may feel overwhelmed when trying to decipher their child’s MRI, leaving them unsure how to interpret the findings on the MRI as they relate to the clinical signs evident in their child. Understanding pontine anatomy and function can assist with interpreting MRI reports, as well as explain the variable clinical symptoms of children diagnosed with DIPG.
General Overview of the Human Nervous System
The human nervous system is divided into the peripheral and central nervous system (CNS). The peripheral nervous system consists of:
- The somatic nervous system: which is responsible for functions under conscious control such as body movement and reception of external stimuli;
- The autonomic nervous system: which regulates functions under subconscious control, such as blood pressure, heart rate, breathing, and digestion.
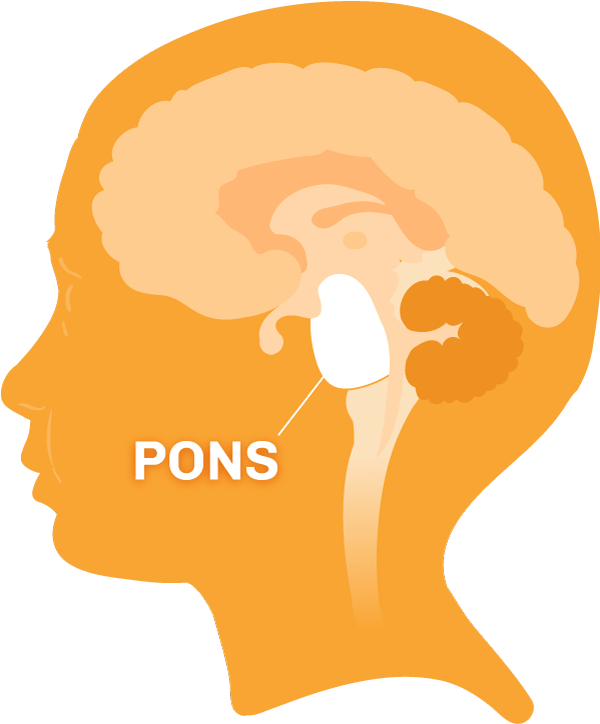
The central nervous system is subdivided into the spinal cord and brain, which includes the cerebrum, cerebellum, and brainstem. The brainstem consists of the midbrain, pons, and medulla and serves as a passageway between the brain and spinal cord. Above the pons is the hypothalamus, and to the back sits the 4th ventricle.
The pons – which means “bridge” in Latin – is an approximately 3.5 cm. long “knob-like” structure that occupies the central portion of the brainstem between the midbrain and the medulla. Any messages descending from the brain or ascending to it must cross this critical “bridge-like” structure.
Neurons and Tracts
To best understand anatomy, it is important to gain an understanding of the terminology of the system being described—in this case the nervous system. The basic cell of the nervous system is the neuron. Humans have billions of neurons, yet neurons only make up approximately 10 percent of cells in the human brain. The remaining 90 percent of cells are support cells called glia.
Neurons
A neuron is composed of dendrites, a cell body, and an axon. Dendrites receive information for the neuron. The information is then passed through the cell body and on to the axon. The axon then passes the information along to dendrites of other neurons. In this way, a neural message gets passed from one neuron to the next. Axons are covered by myelin, which is produced by glial cells and serves as an insulation that allows rapid signal transmission.
Collections of neurons that serve a particular function are called nuclei. Their axons are bundled into collections of thread-like fibers called tracts. Tracts that carry information from the peripheral nervous system up toward the brain are called ascending tracts, while those that carry signals from the brain to the spinal cord and peripheral nervous system are called descending tracts.
Organization of the Pons
The pons consists of a) the basilar pons in the front (ventral portion), and b) the pontine tegmentum in the back (dorsal portion). The basilar pons and the pontine tegmentum contain nuclei and tracts. The basilar pons contains a complex combination of tracts (bundles of axons) and nuclei (collections of cell bodies of neurons). The pontine tegmentum is made up of cranial nerves which serve the head and neck, associated nuclei, the reticular formation (neural network involved in functions including cardiovascular control, pain modulation, sleep and awakening), and tracts (both ascending and descending).
Ascending Tracts of the Pons
The major ascending tracts include the dorsal columns, spinothalamic tracts, and spinocerebellar tracts, which are described below:
Dorsal Columns: The dorsal columns convey information about position sense (proprioception), vibration, and discriminatory touch. Before reaching the pons, the fibers from these columns cross at the level of the lower medulla to form a structure called the medial lemniscus, which then traverses the pons. Damage to the medial lemnisci, at the level of the pons, results in sensory problems on the opposite side of the body.
Spinothalamic Tracts: These tracts convey sensations of pain, temperature, and light touch. The tracts cross shortly after entering the spinal cord and do not change sides as they ascend through the pons. Damage to the spinothalamic tracts, at the level of the pons, results in sensory problems on the opposite side of the body.
Spinocerebellar Tracts: These tracts convey subconscious information pertaining to proprioception (position sense) to the cerebellum, the part of the brain concerned primarily with posture, tone, and balance. These tracts travel to the cerebellum via structures called cerebellar peduncles. Also, there are several nuclei within the pons whose axons unite to form one of the cerebellar peduncles which play a role in the function of the cerebellum. Therefore, damage to these tracts result in problems with posture, tone, and balance.
Descending Tracts
The most important descending tracts of the brainstem include the corticospinal, corticobulbar, and corticopontine fibers, which are described below:
Corticospinal Tracts: These tracts are critical for voluntary movement of the body. They originate from the motor areas of the brain and pass through the basilar pons before crossing at the level of the lower medulla on their way to the spinal cord. Damage to the brain or corticospinal tract at the level of the pons results in weakness or paralysis on the opposite side of the body (remember, these tracts cross to the opposite side in the medulla while on the way to the spinal cord).
Corticobulbar and Corticopontine Tracts: Corticobulbar tracts originate in the brain and control voluntary movement of the muscles of the head and neck. Corticopontine fibers provide a connection between the brain and cerebellum to coordinate and refine movement. These tracts also cross, so damage to corticobulbar fibers result in difficulty moving the opposite side of the face, while lesions of the corticopontine fibers result in lack of coordination of the opposite arm and leg.
Other Tracts
Two other important tracts, which convey both ascending and descending information and are prominent in the pontine tegmentum, are the medial longitudinal fasciculus (MLF) and the central tegmental tract (CTT).
MLF: The MLF is important in coordinating eye, head, and neck movements. Damage to this tract results in problems associated with double vision, and difficulty with coordination of head and eye movements.
CTT: The CTT provides an avenue for ascending tracts involved with taste, as well as provides a path for descending tracts to connect the midbrain to the cerebellum.
Cranial Nerves and Nuclei of the Pons
As previously mentioned, a number of nuclei (groups of cells that serve a particular function) reside within the pons. In the basilar pons (front/ventral portion) reside the pontine nuclei, which serve to connect the brain and cerebellum. Lesions here result in difficulty with coordination of the opposite arm and leg. Cranial nerves are the nerves that control functions of the head and neck, and the pontine tegmentum (back/dorsal portion) contains several of these nuclei.
The lower pons contains cranial nerves (CN) VI and VII. CN VI, known as the abducens nerve, controls a muscle of the eye known as the lateral rectus muscle. This muscle allows the eye to move away from midline toward the temple, a motion known as abduction.
Damage to the nerve results in difficulty abducting the eye on the same side and results in double vision, which is also known as diplopia. The nucleus of the abducens coordinates the lateral rectus muscle of one eye with the medial rectus muscle of the other eye, making it possible to move both eyes to the same side. For this reason, damage to the abducens nucleus results in an inability of both eyes to look toward the side where the tumor is located, rather than the double vision seen in abducens nerve lesions.
CN VII, the facial nerve, also resides in the lower pons. Damage to the facial nerve or its nucleus, results in weakness or paralysis on the same side of the face. Clinically, this manifests as asymmetric facial expressions and can result in difficulty with eating and speaking. Additional important structures that reside in the lower pons include the vestibular nuclei, portions of the spinal trigeminal (the fifth cranial nerve, also called CNV) nucleus and tract, and the superior olivary complex. The vestibular nuclei are involved in balance, so damage here results in dizziness, vertigo, and postural unsteadiness. The spinal trigeminal nucleus and tract mediate pain and temperature sensation from the face. Damage to the spinal CNV nucleus results in sensory disturbances in the face. The superior olivary complex contributes fibers to a structure known as the lateral lemniscus and these structures are involved in hearing. Lesions of the superior olivary complex or lateral lemniscus result in diminished hearing.
The middle portion of the pontine tegmentum is home to three nuclei (called the trigeminal nerve) of CNV—the motor, mesencephalic, and principle sensory nuclei. The motor nucleus controls the muscles that are involved in chewing, while the mesencephalic nucleus is involved with the position sense of these muscles. The principal sensory nucleus is primarily involved with touch sensation from the face. Damage to the motor, mesencephalic, and principle sensory nuclei result in difficulty for the child to coordinate chewing movements, weakness when chewing, as well as facial numbness. The lateral lemniscus that forms in the lower pons, and is involved in hearing continues its ascent through the middle pons. As previously mentioned, damage here results in diminished hearing.
Other Structures Impacting Function of the Pons
Reticular Formation
The reticular formation is a collection of small neural networks that courses through the center of the brainstem, including the midbrain, pons and medulla. It is involved in various functions, including modulation of consciousness, sleep cycles, pain, posture, tone, and balance. Damage to this critical structure can cause sleepiness, coma, and death.
Fourth Ventricle
The brain has ventricles or cavities that naturally produce cerebrospinal fluid (CSF). This fluid circulates throughout the brain acting as a cushion to the nervous system. In a normally functioning brain, this fluid circulates and provides nourishment to the nervous system, and it is subsequently reabsorbed into the bloodstream. If the tumor compresses the 4th ventricle, which is located near the pons, cerebral spinal fluid can build up thereby creating abnormally high pressure within the skull. It is essential that the pressure be relieved so that the tissues in the central nervous system aren’t damaged and the blood flow throughout the brain can be restored. Failure to do so can result in compromised or lost neurological function. Treatment for this fluid buildup—termed hydrocephalus, and also often referred to as “water on the brain,” is most often achieved through the surgical placement of a shunt or an endoscopic third ventriculostomy. As is true with the above mentioned clinical manifestations of DIPG, not all children with DIPG develop hydrocephalus.
Conclusion
An understanding of the anatomy of the pons, the pons function, and the structures it contains provides the framework for deciphering the various neurological deficits that can be seen in patients afflicted with tumors that damage or displace these structures. A number of problems, including weakness, paralysis, numbness, incoordination, hydrocephalus, difficulties with taste, balance, chewing, hearing, vision, and disturbances of consciousness, may occur if these important structures or nearby structures are affected.